
Blog
A failed IVF cycle means that fertilization, embryo development, implantation, or early pregnancy did not progress as expected. IVF failure is medically common and does not mean future treatment will fail. What does reduce future success is repeating IVF without understanding why the previous cycle failed.
This guide explains what to do after a failed IVF cycle, how doctors classify different failure types, what data actually matters, and when repeating IVF is medically reasonable—using clinical logic rather than reassurance. This is the evaluation-first approach followed at Rainbow IVF: analyze first, change strategy second, and proceed only when the data supports it.
No embryos formed → Review egg quality, sperm DNA integrity, and stimulation protocol
Good embryos, no implantation → Reassess transfer timing and endometrial preparation
Pregnancy occurred but ended early → Investigate chromosomal and uterine factors
Multiple failures without explanation → Stop repeating cycles and reassess strategy
This framework prevents emotionally driven decisions and focuses on correct next steps.
IVF success is probabilistic. Even with good embryos and proper transfer, not every cycle results in pregnancy. One failure does not imply poor care or a hopeless prognosis.
The real risk begins when cycles are repeated without changing the underlying variables. Common reasons patients repeat blindly include:
No structured post-cycle review
Overreliance on “everything looked normal”
Pressure to act quickly without clarity
Confusing emotional urgency with medical urgency
A failed IVF cycle should be treated as clinical data. If the cause of failure is unclear, repeating treatment becomes guesswork.
A structured post-failure audit is essential before considering another attempt.
High egg numbers do not compensate for poor egg quality. Review:
Age-related oocyte competence
Response to the stimulation protocol
Egg maturity at retrieval
Indicators of oxidative or structural stress
Increasing medication doses without protocol change often worsens outcomes.
Normal count and motility do not guarantee functional DNA.
Fertilization method used (IVF or ICSI)
Fertilization rate and abnormal fertilization patterns
Indirect indicators of DNA fragmentation
Repeating the same fertilization strategy after failure rarely improves results.
Understanding where development stopped is critical:
Failure to fertilize
Arrest before Day 3
Poor blastocyst formation (Day 5/6)
Each stage suggests a different biological issue. Treating all failures the same leads to repeated disappointment.
Endometrial thickness alone does not ensure implantation.
Hormonal preparation protocol
Synchronization with embryo age
Progesterone exposure timing
Calling the lining “perfect” without timing analysis is misleading.
Embryo transfer and lab handling significantly influence outcomes.
Transfer difficulty or uterine contractions
Catheter placement and timing
Culture conditions and embryo handling
Patients rarely see these factors, but they matter.
Common causes
Declining egg quality
Inappropriate stimulation protocol
Sperm DNA damage
Laboratory stress
What helps
Protocol modification (not escalation)
Addressing sperm-related factors
Egg-quality-focused strategies
What does not
Repeating identical cycles
Random supplements
Attributing repeated failure to luck
This scenario is often oversimplified.
Possible contributors
Embryo–endometrium timing mismatch
Subtle uterine or hormonal factors
Transfer-related issues
Rational next steps
Adjusting transfer timing
Modifying endometrial preparation
Avoiding unnecessary immune or clotting tests without clear indication
This is biologically different from implantation failure.
Possible contributors
Chromosomal abnormalities
Luteal phase support issues
Undetected uterine conditions
Repeating the same approach without investigating miscarriage causes rarely changes outcomes.
Repeating IVF can be appropriate—or harmful—depending on the situation.
A likely cause of failure is identified
The protocol will change meaningfully
Egg or sperm quality is potentially improvable
Time is not a critical limiting factor
Multiple failures occurred with no explanation
Egg reserve is critically low and declining
The plan is simply “try again”
No clear change is planned
More cycles do not automatically increase success if the strategy remains unchanged.
Medically reasonable when:
Egg or sperm quality severely limits embryo development
Repeated cycles show intrinsic gamete issues
Time and age are major constraints
This represents a change in strategy, not a failure.
Useful when:
There is unexplained recurrent pregnancy loss
Maternal age significantly increases chromosomal risk
Less useful when applied routinely without indication or to compensate for poor embryo development.
Sometimes beneficial to:
Reassess physiology
Optimize general health
Avoid rushed decisions driven by anxiety
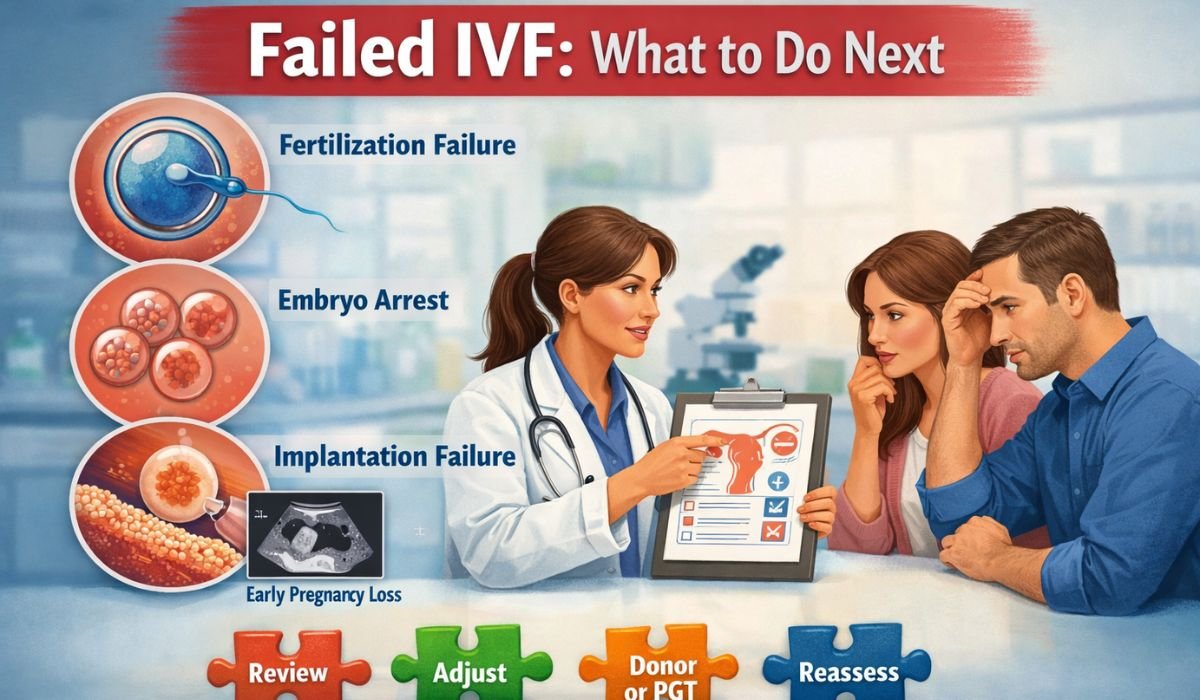
IVF failure usually occurs at one of four stages: fertilization failure, embryo development arrest, implantation failure, or early pregnancy loss. Identifying the exact stage is essential because each requires a different medical response.
A rational next attempt includes at least one strategic change—such as modifying the stimulation protocol, changing fertilization method, adjusting embryo transfer timing, or altering endometrial preparation. Repetition without change rarely improves outcomes.
Objective data matters most: egg maturity and quality, fertilization rates, the stage of embryo arrest, endometrial preparation details, and transfer timing and technique. General reassurance is not a substitute for data.
Reassessment is appropriate after multiple unexplained failures, progressive decline in egg or sperm quality, reuse of the same strategy, or when age and ovarian reserve limit benefit. Reconsidering does not mean stopping—it means changing direction intelligently.
Avoid repeating ineffective elements: the same stimulation protocol after poor egg quality, the same fertilization method after repeated failure, identical transfer timing after implantation failure, or cycles repeated without lab and transfer review.
At Rainbow IVF, failed IVF cycles are approached with:
Detailed cycle audits rather than repetition
Protocol changes based on the identified failure type
Honest counselling that includes discussing limits, alternatives, and timing
The focus is informed decision-making, not cycle count.
What is considered IVF failure?
Failure occurs when embryos do not form, fail to implant, or pregnancy ends in early loss.
How many IVF failures are normal?
One failure is common. Repeated failures require deeper clinical evaluation.
Should IVF be repeated immediately after failure?
Only if a probable cause is identified and the treatment strategy is modified.
Can good embryos still fail to implant?
Yes. Implantation depends on embryo quality, endometrial timing, and transfer technique.
When should donor options be considered?
When repeated cycles show poor embryo development due to egg or sperm factors.
A failed IVF cycle is not the end. Repeating it without analysis often is.
The correct response is not urgency or optimism, but clarity—understanding what failed, what will change, and whether the next step is medically justified.
This content is for educational purposes and does not replace individualized medical consultation.




Ph: +91-562-260-0537, +91-7060301888
Address: Rainbow IVF 4th Floor, Ujala Cygnus Rainbow Hospital, NH-19, Near Guru ka Taal, Gurudwara, Sikandra, Agra, Uttar Pradesh 282007












