
Blog
The Silent Threat to Fertility
Many women do not know they have Pelvic Inflammatory Disease until they struggle to conceive. By the time obvious symptoms appear, significant damage may already be permanent. This infection silently scars the fallopian tubes and surrounding tissues. The result can be blocked fallopian tubes infertility that feels impossible to overcome.
But there is hope. Understanding Pelvic Inflammatory Disease and fertility is the first step toward protecting your reproductive health. This guide explains how PID damages fertility, when to seek help, and how In Vitro Fertilisation can help women with tubal damage become mothers.
Pelvic Inflammatory Disease is a bacterial infection that affects the female reproductive organs, including the uterus, fallopian tubes, and ovaries.
Yes. PID can cause infertility by damaging or blocking the fallopian tubes, making it difficult for sperm and egg to meet. Repeated episodes increase the risk of permanent infertility.
Pelvic Inflammatory Disease is an infection of the upper reproductive tract. The organs affected include:
Uterus (womb)
Fallopian tubes
Ovaries
Surrounding pelvic tissue
How infection spreads
Infection begins in the vagina or cervix. Bacteria travel upward into the uterus, then to the fallopian tubes and ovaries. The body’s inflammatory response causes swelling, tissue damage, and scarring.
Why it often goes unnoticed
Many women experience mild symptoms or no symptoms at all. The infection may persist for months without treatment. By the time a woman notices problems, significant damage has already occurred. This silent progression makes PID particularly dangerous for future fertility.
Learn more about PID symptoms in women and when to seek medical advice.
Understanding the causes of pelvic inflammatory disease helps with prevention.
Sexually transmitted infections
Chlamydia trachomatis and Neisseria gonorrhoeae cause most PID cases. These bacteria spread through unprotected sexual contact. Many women with these infections show no symptoms. Without treatment, the bacteria ascend into the upper reproductive tract.
Poor hygiene and unsafe procedures
Using unclean materials during menstruation can introduce bacteria. Certain medical procedures also carry infection risks, including IUD insertion, abortion procedures, and endometrial biopsy.
Multiple sexual partners
Having multiple partners increases exposure to STIs. Each new partner raises the risk of contracting chlamydia or gonorrhoea.
Bacterial vaginosis
This common vaginal condition alters normal bacterial balance. It creates an environment where harmful bacteria can thrive and ascend upward.
Read more about causes of female infertility and how to reduce your risk.
PID symptoms in women vary widely. Some women experience clear warning signs. Others have no symptoms until infertility becomes apparent.
Mild to moderate symptoms
Lower abdominal pain or tenderness
Unusual vaginal discharge with foul odour
Pain during intercourse
Irregular menstrual bleeding
Fever with chills
Painful or frequent urination
Severe symptoms requiring immediate care
Severe lower abdominal pain
High fever above 101°F (38.3°C)
Nausea and vomiting
Fainting or dizziness
Asymptomatic cases are dangerous
Up to one-third of women with PID have no noticeable symptoms. The infection damages reproductive organs silently. Many women first learn about PID during infertility investigations.
Emotional bridge:
Many women only connect these symptoms to fertility issues when they start trying to conceive, which is often much later.
Routine STI screening may detect underlying infections before PID develops.
For a complete list, refer to our detailed guide on PID symptoms in women.
This is the most important section for understanding Pelvic Inflammatory Disease and fertility. PID damages reproductive structures in several ways.
The fallopian tubes are delicate structures. Their inner lining contains hair-like projections called cilia. These cilia sweep the egg toward the uterus. PID inflammation destroys these cilia permanently. Without functioning cilia, the egg cannot travel through the tube.
Inflammation triggers scar tissue formation. This scar tissue can partially or completely block the fallopian tubes. A completely blocked tube prevents sperm from reaching the egg. It also prevents the fertilised egg from reaching the uterus. Blocked fallopian tubes infertility is one of the most common consequences of PID.
Scarring patterns include proximal blockage (near the uterus), distal blockage (near the ovary), mid-segment blockage, and multiple blockages in both tubes.
Learn more about blocked fallopian tubes infertility and your treatment options.
Partial blockage allows sperm to reach the egg. However, the fertilised egg cannot pass through the narrowed tube. It implants inside the tube instead of the uterus. This is an ectopic pregnancy. Ectopic pregnancies cannot survive. They also pose life-threatening risks to the woman if the tube ruptures.
Women with PID-related damage have significantly higher ectopic pregnancy rates.
The inflammatory response may continue even after the infection clears. This ongoing inflammation can affect egg quality and uterine lining receptivity, reducing pregnancy chances even when tubes remain open.
The answer depends on severity and treatment timing.
Mild PID with early treatment
Women diagnosed and treated promptly have good outcomes. Early antibiotics before significant scarring develops preserve fertility. These women may conceive naturally without assistance.
Moderate PID with some scarring
Some women conceive naturally after treatment. However, pregnancy may take longer. Others require fertility treatments to overcome partial blockages.
Severe PID with extensive damage
Natural conception becomes unlikely. Both tubes may be completely blocked or severely damaged. IVF offers the best chance for pregnancy in these cases.
Realistic outcomes
Do not expect guaranteed pregnancy after PID. Each case differs based on damage extent, age, and overall health. A fertility specialist can assess your individual situation.
Doctors use several methods to diagnose PID:
Pelvic examination – Checks for cervical motion tenderness or uterine pain
Swab tests – Identifies specific bacteria causing infection
Blood tests – Measures white blood cell count and inflammatory markers
Ultrasound – Visualises fallopian tube swelling or fluid collections
Laparoscopy – Direct visualisation of pelvic organs using a small camera
Why early detection matters
Early diagnosis prevents permanent damage. Women with unexplained pelvic pain should seek medical evaluation promptly. Delaying treatment by even a few weeks allows scarring to progress.
Treatment focuses on eliminating infection and preventing further damage.
Antibiotics
Oral antibiotics treat uncomplicated PID. A two-week course is standard. Common combinations include doxycycline with ceftriaxone or metronidazole. Complete the entire course even if symptoms improve.
Hospital treatment
Severe cases require intravenous antibiotics in hospital. Hospitalisation is needed when pregnancy is possible, severe illness with high fever is present, no improvement with oral antibiotics occurs, or an abscess is present in the pelvis.
Surgery
Surgery may be necessary for complications. Tubo-ovarian abscesses may require drainage. Severe scarring might need surgical removal of damaged tissue.
Important limitation
Antibiotics kill bacteria but do not reverse existing damage. Scarred fallopian tubes remain scarred. This is why early treatment is critical.
Damage starts within days of infection. The longer bacteria remain in the upper reproductive tract, the more scar tissue forms. Scarring is permanent. Antibiotics cannot reopen blocked tubes or restore damaged cilia.
Early antibiotic treatment dramatically improves fertility outcomes. Women treated within the first few days of infection have nearly normal pregnancy rates. Those who delay treatment by even a few weeks face significantly higher infertility risks.
If you suspect PID, seek medical care immediately. Do not wait for symptoms to worsen. Early action preserves your future fertility.
Not every PID case causes infertility. However, certain factors increase risk.
Timeline of damage
First episode of PID – 8 to 15 percent become infertile
Second episode – 40 percent become infertile
Third episode – Over 60 percent become infertile
Risk factors for infertility after PID
Delayed diagnosis and treatment
Recurrent PID episodes
Severe infection with abscess formation
Chlamydia as the causative organism
Young age at first infection
Smoking (impairs healing)
For women with blocked or damaged fallopian tubes, IVF offers the most effective path to pregnancy.
How IVF bypasses fallopian tubes
In Vitro Fertilisation completely bypasses the fallopian tubes. The process works as follows:
Eggs are collected directly from the ovaries
Eggs and sperm are combined in a laboratory dish
Fertilisation occurs outside the body
The resulting embryo is placed directly into the uterus
The fallopian tubes play no role in IVF. This makes IVF ideal for PID-related tubal damage.
Who should consider IVF for PID
IVF is recommended when both fallopian tubes are completely blocked, tubes are open but severely damaged, multiple PID episodes have occurred, one year has passed without pregnancy after PID treatment, or an ectopic pregnancy has occurred due to tubal damage.
Micro-CTA:
If you are unsure whether IVF is the right option after PID, getting a proper evaluation can clarify your situation.
Success factors for IVF after PID
IVF success depends on several factors unrelated to tubal damage: the woman’s age at treatment, egg quality and ovarian reserve, uterine health and lining thickness, sperm quality from partner, and lifestyle factors like weight and smoking.
For more details, read our complete guide on IVF treatment for infertility.
IVF success rates for PID patients depend primarily on age and egg quality.
Age-based success per embryo transfer
Under 35 years – 40 to 50 percent pregnancy rate
35 to 37 years – 30 to 40 percent
38 to 40 years – 20 to 30 percent
Over 40 years – 10 to 15 percent
How PID affects these rates
PID does not directly impact the uterus or ovaries in most cases. Therefore, IVF success rates for PID patients mirror general population rates for the same age group. The exception is when PID has caused severe pelvic adhesions affecting ovary access, chronic endometritis (uterine lining infection), or hydrosalpinx (fluid-filled blocked tube).
Hydrosalpinx fluid can leak back into the uterus and harm embryos. Tube removal before IVF improves success rates in these cases.
Realistic expectations
IVF is effective but not guaranteed. Multiple cycles may be needed. Discuss success rates honestly with your fertility specialist based on your specific medical history.
Prevention is always better than treatment.
Safe sexual practices
Use condoms consistently and correctly
Limit number of sexual partners
Get tested regularly for STIs
Ensure partners are tested and treated
Early treatment of infections
Seek treatment immediately for abnormal discharge or pelvic pain
Complete all prescribed antibiotics
Inform partners so they can be treated
Good hygiene practices
Wipe front to back after using the toilet
Avoid douching (disrupts natural bacteria)
Change sanitary pads regularly during menstruation
Regular screening
Sexually active women under 25 should have annual chlamydia screening. Older women with risk factors also benefit from regular testing.
Consider consulting a fertility specialist in these situations:
You have confirmed PID and have been trying to conceive for six months
You have had multiple PID episodes
You have experienced an ectopic pregnancy
You have known blocked fallopian tubes
You have pelvic pain that interferes with daily life
Fertility specialists perform tests to assess tubal status. These include hysterosalpingography (HSG) and laparoscopy. Based on results, they recommend the most appropriate treatment path.
Urgency trigger:
Delaying evaluation after PID can reduce your chances over time. The sooner you understand your tubal health, the more options you have.
Can PID cause permanent infertility?
Yes, PID can cause permanent infertility when it leads to extensive fallopian tube scarring or complete blockage. The damage cannot be reversed with medication or surgery. However, IVF can help women with PID-related infertility achieve pregnancy.
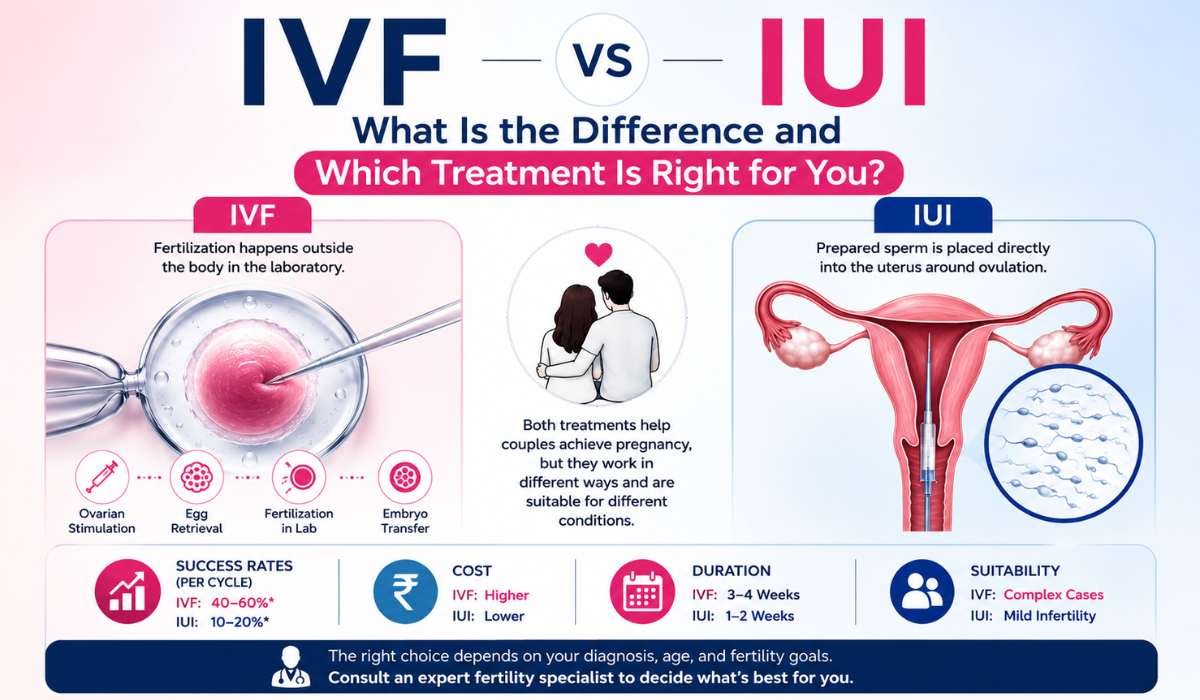
Is IVF necessary after PID?
Not always. Women with mild PID and minimal scarring may conceive naturally. Women with moderate tubal damage may conceive with less invasive treatments like ovulation induction or intrauterine insemination. IVF becomes necessary when both fallopian tubes are completely blocked or severely damaged.
Can PID come back after treatment?
Yes, PID can recur if you are exposed to the same bacteria again. New sexual partners or untreated partners can reintroduce infection. Recurrent PID causes more severe scarring and higher infertility rates. Complete partner treatment and safe sexual practices are essential to prevent recurrence.
How long does it take to conceive after PID treatment?
This varies by damage severity. Women with mild PID may conceive within six to twelve months. Those requiring IVF should begin the process as soon as testing confirms tubal damage. Do not delay seeking help, as age affects IVF success.
Does PID affect egg quality?
PID typically does not directly damage eggs. However, severe pelvic inflammation may affect ovarian function. Chronic infection can sometimes lead to ovarian abscess formation. Tubo-ovarian abscesses may damage ovarian tissue and reduce egg supply.
Can PID cause miscarriage?
PID increases miscarriage risk indirectly through several mechanisms. Chronic endometritis (uterine lining infection) can prevent embryo implantation. Fallopian tube damage increases ectopic pregnancy risk, which cannot survive. Scarring may also affect blood supply to an implanted pregnancy.
What is the best fertility treatment for PID-related blocked tubes?
IVF is the most effective treatment for women with blocked fallopian tubes from PID. It completely bypasses the damaged tubes. Success rates are comparable to women without PID in the same age group. For unilateral blockage (only one tube blocked), natural conception or less invasive treatments may still work.
Understanding PID and fertility is important, but taking action at the right time matters more. If you have had PID and are struggling to conceive, early evaluation can help you move in the right direction.
The next step is to get your fertility evaluated at the right time. You can take this step by filling out the contact form on our Contact Us page. Our team will review your details and guide you on the next steps.

Ph: +91-562-260-0537, +91-7060301888
Address: Rainbow IVF 4th Floor, Ujala Cygnus Rainbow Hospital, NH-19, Near Guru ka Taal, Gurudwara, Sikandra, Agra, Uttar Pradesh 282007












